Articles
- Page Path
- HOME > Res Community Public Health Nurs > Volume 34(3); 2023 > Article
-
Original Article
노인의 이중 감각 저하가 인지기능 저하에 미치는 영향: 사회적 지지의 조절효과 -
양수지1
 , 윤주영2
, 윤주영2 - The Effect of Dual Sensory Impairment on Cognitive Function Decline in the Elderly: The Moderating Effect of Social Support
-
Soo Jee Yang1, Ju Young Yoon2
-
Research in Community and Public Health Nursing 2023;34(3):217-227.
DOI: https://doi.org/10.12799/rcphn.2023.00255
Published online: September 27, 2023
1서울대학교병원 간호사
2서울대학교 간호대학 교수
1Registered Nurse, Seoul National University Hospital, Seoul, Korea
2Professor, College of Nursing, Seoul National University∙Research Institute of Nursing Science, Seoul National University∙Center for Human-Caring Nurse Leaders for the Future by Brain Korea 21 (BK 21) four project, College of Nursing, Seoul National University, Seoul, Korea
- Corresponding author: Ju Young Yoon PhD, RN, Professor, College of Nursing and Research Institute of Nursing Science, Seoul National University, 103 Daehak-ro, Jongno-gu, Seoul 03080, South Korea Phone: +82-2-740-8817, Fax: +82-2-741-5244, Email: yoon26@snu.ac.kr
Copyright © 2023 Korean Academy of Community Health Nursing
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License. (http://creativecommons.org/licenses/by-nd/4.0) which allows readers to disseminate and reuse the article, as well as share and reuse the scientific material. It does not permit the creation of derivative works without specific permission.
- 1,336 Views
- 44 Download
Abstract
-
Purpose
- This study verified that the dual sensory impairment (DSI) in the elderly is associated with cognitive impairment (CI) and confirmed how change in cognitive function varies depending on the social support (SS).
-
Methods
- For a study sample of Korean older people, data from the Korean Longitudinal Study of Ageing (KLoSA) from the 7th (2018) to the 8th (2020), were included in this cross-sectional descriptive study. Among people who responded in both 2018 and 2020, a total of 2,069 people of those who are 65 years of age or older, and have living children and normal cognitive function, were analyzed. X2 -test, t-test and logistic regression analyses were utilized.
-
Results
- First, the number of elderly with visual impairment (VI), hearing impairment, and DSI increased on 8th data compared with 7th data. In addition, 22.9% of the 2,069 people showed a decrease in cognitive function. Second, compared to the elderly with normal sensory function, the cognitive function of the elderly with only VI was found to be more degraded, and the cognitive function of the elderly with DSI was found to be much more degraded. In addition, among SS, only participation in social gatherings was found to show significant change in cognitive function of the elderly with DSI. Third, the interaction effect of participating in social gatherings was not significant in the CI of the elderly with DSI.
-
Conclusion
- VI and DSI effected cognitive function, but participation in social gatherings such as SS has not significant interaction effect on CI of the elderly with DSI.
- 국내 65세 이상 노인 인구의 연평균 증가율이 3.3%로 OECD 국가 중 가장 빠르게 고령화 속도가 진행되어 고령사회 진입했으며[1], 2020년 기준 고령자 가구가 전체 가구의 22.8%를 차지하고 있다[2]. 따라서 노화로 인한 감각 기능 저하를 겪는 노인들의 수도 급증하고 있으며, 노인들의 감각 저하는 둘 이상의 감각이 동시에 저하되는 특징이 있다[3]. 한국 코호트 연구에 따르면, 58세 이상인 노인 6520명 중 약 15%가 감각이 정상인 반면, 약45%가 단일 감각 저하를, 약 40%가 이중 감각 저하를 가지고 있었다[4]. 감각 저하가 있는 노인은 의사소통 제한으로 사회활동 기회가 줄어들면서 외로움을 느꼈고[5] 인지기능저하[6-9]까지 경험하게 된다.
- 인지기능 저하를 진단받은 경우 50% 이상이 5년 이내에 치매로 진행되므로[10], 인지기능 저하의 조기 예방 중요성을 강조되어 관련된 연구가 많이 진행되었다. 그러나 이중 감각 저하가 노인에게 빈번하게 발생할 수 있는 신체 노화 증상임에도 불구하고 단일 감각 저하 또는 증상 조절과 인지기능 간의 관계 연구 위주로 진행되었고[11-14], 심지어 감각 저하 증상을 위한 치료적 중재에는 경제적 한계가 따른다. 시력 보조장치와 인지기능에 대한 선행 연구가 없어 우울과 관련된 연구를 보면, 시력 저하가 있는 경우 시력 보조장치가 우울정도에 영향을 미치지 않으나, 시력저하 관련 상담이 우울정도 감소에 도움되는 것으로 나타났다[15]. 반면 청력 저하가 있는 경우 보청기 착용이 의사소통 문제를 줄이고 우울 증상을 개선시키며[16] 인지기능에 도움이 되었으나[14], 청력저하가 있는 노인의 70~85%가 보청기를 처방 받지 않았고, 처방을 받더라도 절반도 안 되는 노인이 보청기를 사용하지 않는다고 나타났다[17,18]. 그 이유는 개인의 청력 손실을 과소평가하거나 불편감, 비용 때문이었다[19,20]. 게다가 감각 저하 증상 조절과 관련된 경제적 한계 측면을 보면, 한국의 노인 빈곤율은 OECD평균의 3배인 43.4%로 개인의 경제적 어려움이 상대적으로 클 뿐만 아니라[21], 저하된 감각 기능 조절을 위한 중앙 정부 및 지자체의 예산이 충분하지 않아 지원받을 수 있는 대상자는 제한적이다[22,23].
- 이러한 한계를 보완하기 위해 본 연구는 사회적 지지를 저하된 감각 기능에 대한 예산에 부담이 있을 때 대체적 중재로서 활용하고자 한다. 가족과 이웃 같은 커뮤니티를 통한 사회적 지지는 큰 예산상 지원 없이 확보가 가능하여 비용 효율적이기 때문이다. 사회적 지지의 효과를 확인하기 위해 선행연구를 보면, 사회적 지지인 배우자와 이혼하거나 과부 또는 홀아비인 노인에게 치매 발생 가능성이 높았고[24] 자녀와의 접촉이 많을수록 인지기능 저하될 확률이 낮은 것으로 나타났다[25]. 그리고 사회 통합 참여를 할수록 인지기능 저하될 확률이 낮았다[26]. 뿐만 아니라 도구적 지지로서 세대 간 금전교류가 없거나 받기만 한 경우 인지기능이 감소되었고, 노인이 자녀에게 선물, 여행과 같은 비금전적 지원을 해주는 경우와 인지기능 간의 연관성이 있었다[27].
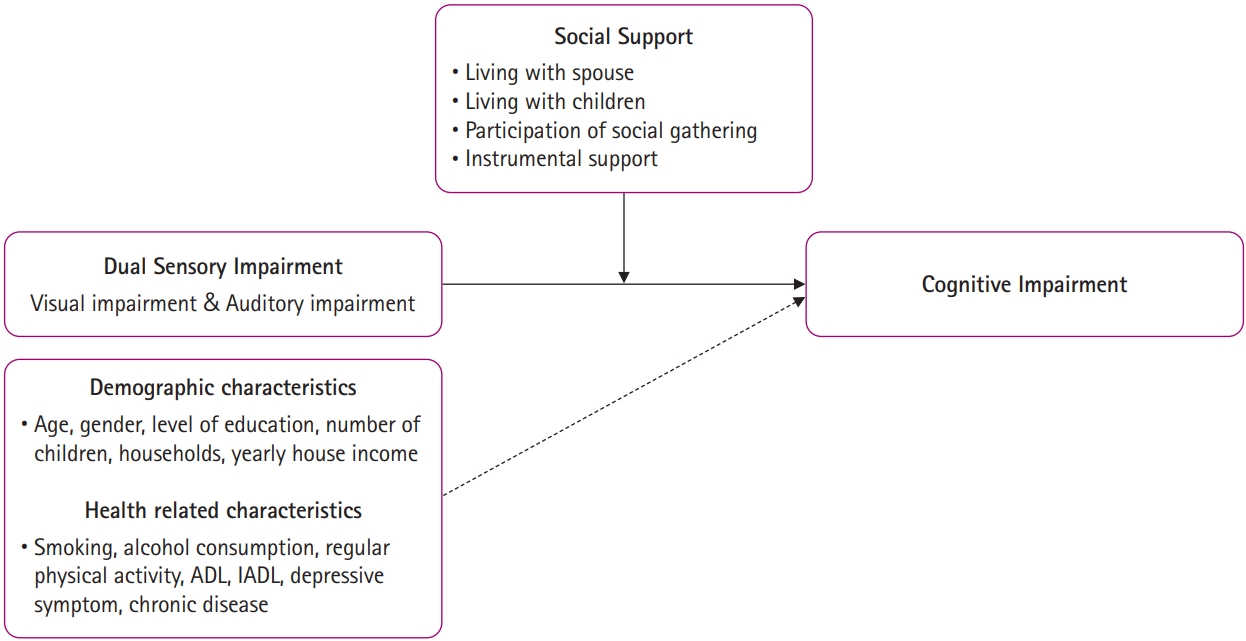
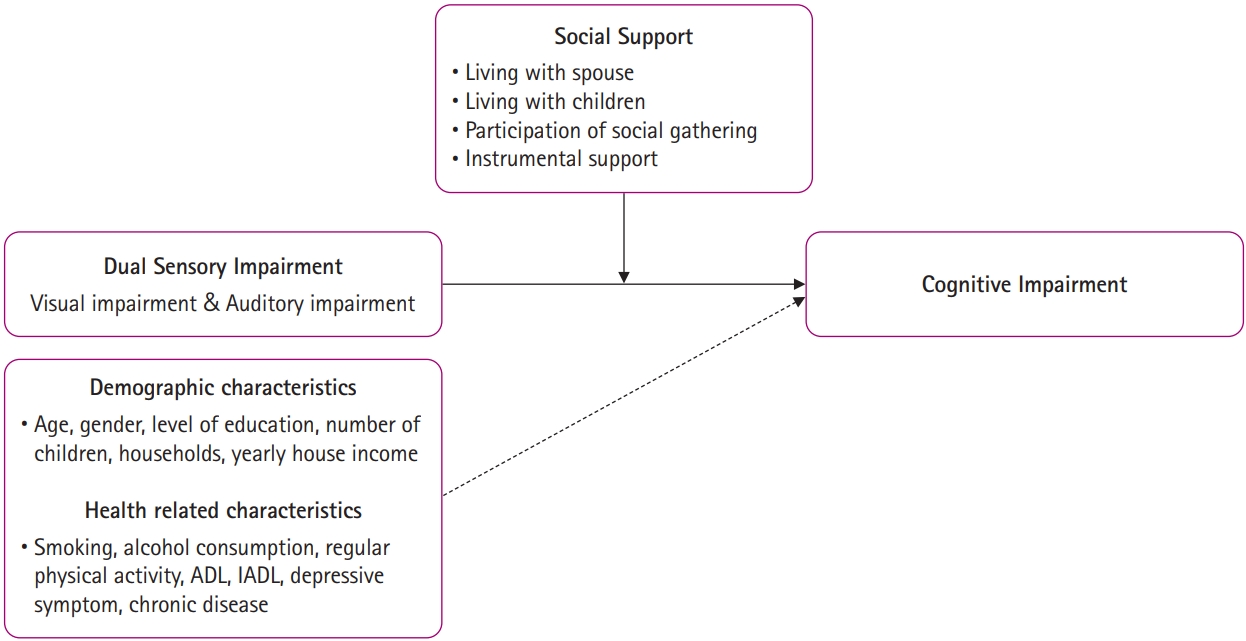
- 따라서 본 연구에서는 지역사회에 거주하는 전체 노인 중 이중 감각 저하가 있는 노인이 2년 후 인지기능 악화에 어떤 영향을 미치는지 파악하고, 사회적 지지의 수준이 이중 감각 저하와 인지기능 악화에 조절효과가 있는지 확인하고자 한다. 이를 위해 본 연구는 Verbrugge & Jette [28]의 장애과정모델을 기반으로, 병리적 특성과 손상을 하나로 묶어 이중 감각 저하를 한단계로 설정하고, 이중 감각 저하에 따른 신체적 또는 정신적 제한을 기능 제한 단계, 인지기능 저하를 장애 단계인 3단계로 수정 보완하여 구성하였다. 그리고 위험요인으로는 인구사회학적 요인, 내적요인은 건강 관련 특성, 외적 요인은 사회적 지지로 설정하였다(Figure 1).
서 론
- 1. 연구 설계
- 본 연구는 한국고용정보원 포털 홈페이지(https://survey.keis.or.kr/)에서 제공한 7차(2018년), 8차(2020년) 고령화연구패널조사(Korean Longitudinal Study of Ageing, KLoSA)를 활용한 이차자료 분석연구로, 시력과 청력이 동시에 저하가 되는 이중 감각 저하가 있는 65세 이상의 노인을 대상으로 인지기능의 변화를 확인하고, 사회적 지지가 인지기능 변화에 미치는 조절효과를 파악하기 위한 서술적 상관관계 연구이다. 본 연구에서는 2018년에 응답한 대상자에서 65세 이상이고 인지기능에 문제가 없고 사회적 지지가 되는 동거 또는 비동거 하는 생존 자녀가 있는 대상자 중, 2020년에 응답하지 않은 경우를 제외하여 총 2069명을 분석하였다.
- 2. 연구 도구
- 2018년 고령화연구패널조사의 문항에서 시력, 청력에 대한 자가 평가하는 도구를 통하여 감각 기능 저하 여부를 분류하였다. 시력을 자가 평가하는 문항으로 ‘시력(교정시력 포함)은 어떻습니까?’과 청력을 자가 평가하는 문항은 ‘청력은 어떻습니까? 보청기를 사용하시는 경우는 보청기를 낀 상태를 말씀해 주십시오.’이다. 이 문항에 대한 응답은5점 Likert 척도로, 5점은 ‘매우 나쁨’, 4점은 ‘나쁜 편’, 3점은 ‘보통’, 2점은 ‘좋은 편’, 1점은 ‘매우 좋음’으로 스스로 시력과 청력 정도를 측정한다. 따라서 본 연구에서 ‘이중 감각 저하’란 시력과 청력에 대한 자가 평가 문항에 모두 4점 이상으로 나쁜 편 또는 매우 나쁨이라고 응답한 경우를 의미한다.
- 인지기능 측정에 사용되는 한국어판 간이정신상태 검사(Korean version of Mini-Mental State Examination: K-MMSE)는 총 점수 범위는 0-30점으로, 그 중 24점 미만일 때 인지기능 저하로 평가된다[29]. 본 연구에서는 2018년에는 인지기능 점수가 24점 이상으로 인지기능이 정상인 노인을 분석집단으로 포함하였으며, 2년 후인 2020년 인지기능 점수 중 24점 미만이 된 대상자를 ‘인지기능 저하'로, 24점 이상인 대상자를 ‘인지기능 유지’로 범주화 하였다.
- 사회적 지지는 감정, 관심과 같은 정서적 지지, 물질적 도움인 돈 또는 시간과 같은 도구적 지지, 긍정적인 자기 평가 및 수용과 같은 평가적 지지, 정보와 충고와 같은 정보적 지지로 구분한다[30]. 본 연구에서도 사회적 지지를 4가지로 구분하여 설정하려고 하였으나 고령화연구패널조사 데이터의 한계로, 배우자 또는 동거 자녀 유무, 사회모임 참여 여부, 도구적 지지로 세대 간 금전/비금전 지원 및 수령 여부로 사회적 지지를 설정하였다. 먼저 동거 가족 유무 및 사회모임 참여여부가 정서적 지지를 상징하기 어려워 따로 분류하였다. 그리고 사회적 지지를 받는 것으로만 정의하는 것은 전통적인 방향이고 최근에는 사회적 지지는 받는 것뿐만 아니라 제공하는 것도 동일한 이득이 생긴다는 인식이 증가하고 있어[31,32], 자녀와 부모 사이에 금전 또는 비금전을 주거나 받았는지에 대한 것을 도구적 지지로 설정하였다. 평가적, 정보적 지지로 측정할 수 있는 항목은 고령화연구패널조사 데이터에 존재하지 않아 사회적 지지로 설정하지 못하였다.
- 배우자와의 동거여부는 고령화연구패널조사의 2018년 자료 중 최종 혼인상태 관련 문항에 대한 응답에서 혼인 중을 0, 별거나 이혼, 사별과 같은 그 외를 1로 범주화 하였다. 자녀와의 동거여부는 고령화연구패널조사의 2018년 자료 중 첫째부터 아홉째 자녀와 현재 함께 살고 있는지 확인하는 문항을 활용하여 자녀 한명이라도 동거하고 있으면 0, 없으면 1로 범주화 하였다.
- 고령화연구패널조사의 2018년 자료 중 참여하고 있는 사회모임을 확인하는 문항에서 종교 모임, 친목 모임, 문화 관련단체, 동창회, 봉사모임, 시민단체 등과 같은 항목에 하나라도 참여한 경우는 0, 하나도 참여하지 않은 경우를 1로 범주화 하였다.
- 도구적 지지는 고령화연구패널조사의 2018년 자료 중 자녀(동거와 비동거)에게 금전(용돈 및 생활비)과 비금전(여행 및 선물) 자원을 제공하거나, 자녀로부터 금전과 비금전 자원을 수령하는 것으로 측정하였다. 금전 교류 여부는 첫째부터 아홉째 자녀까지 “작년 한 해 동거/비동거 자녀와 정기적/비정기적으로 용돈과 같은 금전적 지원을 하셨습니까/받으셨습니까?”라는 문항에서 교류를 하는 경우(지원 또는 수령 둘 중에 하나라도 하는 경우 포함), 아예 교류가 없는 경우로 나누었다. 비금전 교류 여부 확인을 위해, 첫째부터 아홉째 자녀까지 “작년 한 해 동거/비동거 자녀와 정기적/비정기적으로 현물과 같은 비금전적 지원을 하셨습니까/받으셨습니까?”라는 문항에서 교류를 하는 경우(지원 또는 수령 둘 중에 하나라도 하는 경우 포함), 아예 교류가 없는 경우로 나누었다. 이렇게 금전 또는 비금전으로 구분한 자료의 자녀로부터 수령 또는 지원과 관련된 척도에서 지난 1년 동안 정기적/비정기적으로 수령 또는 지원받는 경우를 1, 그렇지 않은 경우를 0으로 범주화 하였다.
- 고령화연구패널조사의 2018년 자료에서 인구사회학적 특성을 성별과 연령, 교육수준, 생존자녀(수), 세대구성, 경제수준(가구총소득)으로 구성하고, 건강 관련 특성을 생활습관(흡연, 음주), 운동, ADL(Activities of Daily Living), IADL(Instrumental Activities of Daily Living), 우울점수, 만성질환 수로 구성하여 통제하였다[33-41].
- 3. 자료 분석 방법
- 본 연구에서는 7차(2018년), 8차(2020년) 고령화연구패널조사 표본을 SPSS 29.0프로그램을 사용하여 다음과 같이 분석하였다.
- 1) 지역사회에 거주하는 인지기능이 정상이고 자녀가 있는 노인들의 일반적 특성을 파악하기 위해 기술통계 실시하여 평균, 표준편차, 빈도, 백분율을 분석하였다.
- 2) 감각 기능이 정상인 노인과 단일 감각 저하와 이중 감각 저하가 있는 노인의 인지기능의 차이를 비교하기 위해 t-test, χ2 test 와 같은 차이검정을 분석하였다.
- 3) 이중 감각 저하 여부가 2년 후 인지기능 저하에 영향을 미치는지 파악하기 위하여 인지기능에 영향을 미치는 다른 요인을 보정한 후 다중 로지스틱 회귀분석을 분석하였다.
- 4) 이중 감각 저하와 인지기능 저하와의 관계에서 사회적 지지의 조절효과를 보기 위하여 상호작용 변수를 추가하여 다중 로지스틱 회귀분석을 실시하였다.
- 4. 윤리적 고려 사항
- 서울대학교 생명윤리위원회의 ‘연구 대상자 보호 심사위원회 면제’ 심의 승인을 받은 후 시행하였다(IRB No. E2303/002-003).
연 구 방 법
1) 독립변수: 이중 감각 저하
2) 종속변수: 인지기능
3) 조절변수: 사회적 지지
(1) 배우자 또는 동거 자녀 유무
(2) 사회모임 참여 여부
(3) 도구적 지지: 세대 간 금전/비금전 지원 및 수령 여부
4) 통제 변수
- 1. 연구대상자의 일반적 특성
- 분석 대상자 총 2069명의 일반적 특성은 Table 1과 같다. 7차(2018년)에는 인지기능 점수가 24점 이상으로 정상인 노인 중 473명이 8차(2020년)에 23점미만으로 인지기능이 저하가 되었다. 그리고 건강 관련 특성에서 이중 감각 저하가 있는 노인은 2018년에는 2.7%에서 2020년에는 2.9%로, 시력 저하가 있는 노인은 13.9%에서 15.8%로 청력 저하가 있는 노인은 4.0%에서 5.8%로 증가하였다. 반면 사회적 지지와 관련된 특성에서는 배우자가 있는 경우가 2018년에는 77.1%에서 2020년에는 74.1%로, 자녀와 동거하는 경우도 20.6%에서 18.6%로 감소하였다. 사회모임 참여 개수도 1.09±0.73개에서 0.94±0.78개로 감소하였다. 그리고 사회적 지지 중 도구적 지지인 세대간 금전 교류가 있는 경우도 25.6%에서 19.6%로, 비금전 교류가 있는 경우는 31.8%에서 27.4%로 감소하였다(Table 1).
- 2. 일반적 특성에 따른 인지기능 악화의 차이 분석
- 본 연구대상자의 일반적 특성에 따른 인지기능 악화의 차이를 χ2과 t-test를 실시하여 분석한 결과는 Table 2와 같다. 대상자의 인구 ∙ 사회학적 특성 중 연령, 성별, 교육수준, 생존자녀 수, 세대구성, 가구 총소득에 따라 인지기능 악화에 유의한 차이가 있는 것으로 나타났다. 인지기능이 악화된 노인의 평균 연령은 인지기능이 유지된 노인에 비해 약 3세 높았고 여성 노인 비율은 남성 노인 비율보다 인지기능 악화 비율이 높았다. 교육 수준에서 6년 이하 교육을 받은 경우가 6년 이상 교육받은 경우에 비해 인지기능이 악화되는 비율이 높았다. 인지기능이 악화된 노인이 유지된 노인에 비해 생존 자녀수가 많았고 세대 구성 중 독거세대 비율이 높았다. 가구 총 소득에서 인지기능이 악화된 노인의 소득이 인지기능이 유지된 노인의 소득에 비해 약 6백 7십만원이 낮았다.
- 건강 관련 특성과 인지기능의 변화를 살펴본 결과, 흡연, 음주, 운동, IADL, 우울점수, 만성질환 수, 감각 저하가 유의하게 나타났다. 인지기능이 악화된 노인이 유지된 노인에 비해 흡연과 음주를 하는 비율이 낮았다. 그러나 인지기능이 악화된 노인이 유지된 노인에 비해 수단적 일상생활수행능력에 독립적이지 않은 비율이 높은 것으로 나타났다. 그리고 우울 점수는 인지기능이 악화된 노인이 유지된 노인에 비해 약 1.9점 높았고, 만성질환 수도 약 0.4개 많았다. 인지기능이 악화된 노인이 유지된 노인에 비해 이중 감각 저하, 시력 저하, 청력 저하가 있는 비율이 높은 것으로 나타났다.
- 사회적 지지와 관련된 특성과 인지기능의 변화를 확인한 결과, 배우자 여부, 사회모임 참여 여부, 세대 간 금전교류가 통계적으로 유의하다고 나타났다. 인지기능이 악화된 노인이 유지된 노인에 비해 배우자와 함께 살지 않는 비율이 높았고, 사회모임에 참여하지 않는 비율도 높았다. 반면 세대간 금전 교류를 하지 않는 노인은 교류하는 노인에 비해 인지기능 악화 비율이 낮았다(Table 2).
- 3. 감각 저하와 사회적 지지가 인지기능 저하에 미치는 영향
- 감각 저하와 사회적 지지가 인지기능 저하에 미치는 영향을 검증하기 위해, 다른 영향 요인인 일반적인 특성과 건강관련 특성을 보정한 후 다중 로지스틱 회귀분석으로 분석한 결과는 Table 3의 Model A와 같다(Table 3). 시력만 저하된 노인인 경우, 감각 기능이 정상인 노인에 비해 인지기능이 저하가 될 확률이 1.68배(95% CI: 1.24, 2.28) 높았으며, 이중 감각 저하가 있는 노인인 경우 인지기능 저하가 발생할 확률은 2.89배(95% CI: 1.56, 5.33) 높았다. 시력만 저하가 된 노인보다 이중 감각 저하가 있는 노인이 인지기능 저하될 확률이 더 높은 것으로 나타났다. 사회적 지지 관련 특성을 분석한 결과, 사회모임에 참여를 하지 않은 경우가 사회모임을 참여하는 경우보다 인지기능이 저하될 확률이 1.49배(95% CI: 1.11, 1.98) 높은 것으로 나타났다.
- 4. 이중 감각 저하와 인지기능 사이 사회적 지지의 조절효과
- 본 연구는 노인의 이중 감각 저하에 따른 인지기능 변화에서 다른 영향 요인들을 보정한 후, 인지기능 변화에 유의했던 사회적 지지인, 사회모임 참여여부의 조절효과를 검증하기 위해 다중 로지스틱 회귀분석을 수행하였고 결과는 Table 3의 Model B와 같다. 사회모임 참여 여부는 이중 감각 저하가 있는 노인의 인지기능 변화에 조절효과가 나타나지 않았다.
연 구 결 과
- 본 연구는 고령화연구패널조사(KLoSA) 자료를 이용하여 노인의 이중 감각 저하가 인지기능에 미치는 영향과 사회적 지지의 조절효과를 파악하고자 하였다.
- 감각 기능이 정상인 노인에 비해 시력만 저하된 노인은 인지기능 저하가 발생할 확률이 1.68배 높았으나 이중 감각 저하가 있는 노인은 2.89배 더 높은 것으로 나타나, 미국의 코호트 연구의 연구결과와 일치하였다[42]. 다만, 본 연구에서는 청력 저하만 있는 노인의 경우 인지기능 저하 발생 확률이 유의미하게 높아지지 않았는데 이는 위의 선행 연구 결과와 상이하였다[42]. 상이한 결과가 발생한 원인에 대해 추정하면, 시력 저하가 있는 노인은 2년 동안 추적 관찰한 결과 인지기능 저하가 될 가능성이 크다는 선행 연구[43,44]가 진행된 것에 비해, 청력 저하가 있는 노인의 인지기능 같은 경우 5년 또는 그 이상의 기간 동안 추적관찰 결과 인지기능 저하 또는 치매 발병률이 높다는 논문이 상대적으로 많았다[45-47]. 본 연구는 2년 간격의 단기간 연구이기 때문에 청력 저하와 인지기능 저하 간의 관계에 대한 입증이 어려웠던 것으로 판단된다. 따라서, 양자 간의 관계에 대한 정확한 분석을 위해서는 시력 저하가 있는 노인에 비해 청력 저하가 있는 노인의 경우 감각 저하가 인지기능에 영향을 주는 기전이 상대적으로 지연되는 점을 고려하여 장기간의 추적 관찰이 있어야 할 것이다.
- 사회적 지지에 따른 인지기능 변화에 대한 검증에서, 사회모임을 하나도 참여하지 않은 노인은 하나라도 참여하는 노인에 비해 인지기능이 저하될 확률이 높은 것으로 나타나, 사회적 활동을 하지 않는 것이 낮은 인지기능과 관련 있다는 선행연구를 뒷받침할 수 있었다[48]. 그러나 사회모임 참여 여부의 조절효과는 유의하지 않은 것으로 나타났다. 이 결과는 이중 감각 저하가 있는 노인이 의사소통에 어려움을 겪고 있어 사회모임에 적극적으로 참여하지 못하고, 사회모임에 참여를 하더라도 의사소통 제한으로 우울 증상이 나타나 오히려 부정적으로 작용하여[49] 사회모임 참여의 조절효과를 입증하는데 제한이 있었을 것으로 생각된다. 따라서 사회모임 참여 여부 뿐 아니라 사회모임 참여 정도와 질에 관련한 추후 연구가 필요하다.
- 많은 선행 연구에서 노인의 인지기능 저하에 미치는 요인이 증명되었으나[33-41], 인지기능 저하를 예방할 수 있는 역동적 요인을 조절효과로 분석하는 연구는 미비한 실정이다. 따라서 본 연구는 감각 기능 저하 별 인지기능 저하 정도를 확인하고 인지기능 저하를 예방할 수 있는 차별화된 중재개발을 위해 진행되었다. 하지만 사회적 지지의 조절효과를 입증하기에는 다음과 같은 제한점이 있었다. 첫째, 7차(2018년), 8차(2020년) 두 시점만 활용해 청력 저하가 있는 노인의 인지기능 변화까지 입증하는데 제한 있었고, 이중 감각 저하 대상자 수가 충분치 않아 사회모임 참여의 조절효과 검증에 한계가 있었다. 둘째, 시력과 청력을 자가 평가하여 객관성이 낮은 측면이 있다. 셋째, 본 연구는 사회적 지지의 질적인 부분인 심리 ∙ 정서적인 면을 고려하지 않았다. 넷째, 고령화연구패널조사는 지난 1년간의 과거를 회상하여 측정하는 설문조사로 설문자에게 더 나은 모습을 보여주기 위해 회상 비뚤림(recall bias)이 있을 수 있어 실제로는 세대 간 교류가 없었는데 있었다고 응답하는 비율이 높이는 방향으로 작용되었을 수 있다. 마지막으로, 사회적 지지의 경우 시간이 지남에 따라 변화 가능성이 많은데 본 연구에서는 이런 역동적인 특성을 고려하지 않은 것에 한계가 있다.
논 의
- 본 연구는 인지기능이 정상이고 자녀가 있는 65세 이상인 이중 감각 저하가 있는 노인의 인지기능에 미치는 영향과 사회적 지지의 조절효과를 알아보았다. 노인의 시력 저하와 이중 감각 저하는 인지기능 저하에 유의한 영향을 미쳤으나 청력 저하는 유의하지 않았다. 그리고 사회적 지지인 사회모임 참여 여부는 인지기능 저하에 대한 영향 요인으로 검증되었지만, 이중 감각 저하가 있는 노인의 인지기능 저하를 예방하기 위한 중재로 활용하기 위한 조절효과 검증에는 유의하지 않은 것으로 나타났다.
- 본 연구결과를 토대로 지역 사회 간호 적용에 있어 다음과 같은 제언을 하고자 한다.
- 첫째, 두 시점보다 많은 시점의 자료를 사용하는 것이 더욱 안정적일 것으로 생각된다.
- 둘째, 신체검진과 같은 객관적인 시력 및 청력 사정 자료를 활용할 수 있다.
- 셋째, 사회적 지지에서 만족도와 같은 질적인 측면을 고려할 필요가 있다.
- 넷째, 변화 가능성이 높은 사회적 지지를 고려하여, 복합 표본 분석을 할 필요가 있다.
결 론
-
Conflict of interest
Ju Young Yoon is an editorial board member of the Journal of Korean Community Health Nursing. She will not involve in the review process of this manuscript. No conflict of interest has been declared by authors.
-
Funding
The author(s) disclosed the following financial support for the research, author, or publication of this article: This work was supported a scholarship, called Hanmaeum scholarship, from the Seoul Nurses Association in 2022 to foster nursing researchers’ talent in the nursing community and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2022R1I1A207290712).
-
Authors’ contributions
Soo Jee Yang contributed to conceptualization, data curation, formal analysis, methodology, project administration, and writing – original draft, review & editing. Ju Young Yoon contributed to conceptualization, methodology, supervision, validation, and writing – review & editing.
-
Data availability
The survey data were collected from Korea Longitudinal Study on Aging(KLoSA). Detail information about the data is available on the KLoSA website (https://survey.keis.or.kr/index.jsp).
NOTES
Acknowledgments
Note. Yearly household income unit is in 1,000,000 Korean won, which approximately equals US $100.; ADL means activities of daily living.; IADL represented instrumental activities of daily living.; Depressive symptoms were measured in using the Center for Epidemiologic Studies Depression(CES-D10).; Cognitive function is assessed in this study using the Korean Version of the Mini Mental Stated Examination(K-MMSE).; Chronic diseases included hypertension, diabetes mellitus, cancer, chronic pulmonary disease, liver disease, heart disease, cerebrovascular diseases, psychiatric disorder, arthritis or rheumatism, prostate disease, digestive system disease, slipped disk and dementia.; Regular physical activity indicated physical activity once a week.; Monetary support included allowance and living expenses.; Non-monetary support included gifts, trips, electronics, and supplement foods.
Note. Yearly household income unit is in 1,000,000 Korean won, which approximately equals US $100.; ADL means activities of daily living.; IADL represented instrumental activities of daily living.; Depressive symptoms were measured in using the Center for Epidemiologic Studies Depression(CES-D10).; Cognitive function is assessed in this study using the Korean Version of the Mini Mental Stated Examination(K-MMSE).; Chronic diseases included hypertension, diabetes mellitus, cancer, chronic pulmonary disease, liver disease, heart disease, cerebrovascular diseases, psychiatric disorder, arthritis or rheumatism, prostate disease, digestive system disease, slipped disk and dementia.; Regular physical activity indicated physical activity once a week.; Monetary support included allowance and living expenses.; Non-monetary support included gifts, trips, electronics, and supplement foods.
- 1. Statistics Korea. Life expectancy at birth and disability adjusted life expectancy [Internet]. Daejeon: Statistics Korea. 2021 [cited 2023 Jan 3]. Available from: https://www.index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd=2758
- 2. Statistics Korea. Population projections for Korea [Internet]. Daejeon: Statistics Korea. 2019 [cited 2023 Jan 3]. Available from: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B040M5&conn_path=I3
- 3. Correia C, Lopez KJ, Wroblewski KE, Huisingh-Scheetz M, Kern DW, Chen RC, et al. Global sensory impairment in older adults in the United States. Journal of the American Geriatrics Society. 2016;64(2):306–313. https://doi.org/10.1111/jgs.13955ArticlePubMedPMC
- 4. Byeon G, Oh GH, Jhoo JH, Jang JW, Bae JB, Han JW, et al. Dual sensory impairment and cognitive impairment in the Korean longitudinal elderly cohort. Neurology. 2021;96(18):e2284–e2295. https://doi.org/10.1212/wnl.0000000000011845ArticlePubMed
- 5. Mick P, Parfyonov M, Wittich W, Phillips N, Guthrie D, Kathleen Pichora-Fuller M. Associations between sensory loss and social networks, participation, support, and loneliness: Analysis of the Canadian longitudinal study on aging. Canadian Family Physician Medecin de Famille Canadien. 2018;64(1):e33–e41. PubMedPMC
- 6. Bae SH, Kim GY. The association between self-reported sensory impairment and cognitive function among Korean older adults: Results from the 2017 national survey of the living conditions and welfare needs of older Koreans. Journal of the Korean Gerontological Society. 2019;39(2):389–404. http://doi.org/10.31888/JKGS.2019.39.2.389Article
- 7. Davidson JGS, Guthrie DM. Older adults with a combination of vision and hearing impairment experience higher rates of cognitive impairment, functional dependence, and worse outcomes across a set of quality indicators. Journal of Aging and Health. 2019;31(1):85–108. https://doi.org/10.1177/0898264317723407ArticlePubMed
- 8. Hong T, Mitchell P, Burlutsky G, Liew G, Wang JJ. Visual impairment, hearing loss and cognitive function in an older population: Longitudinal findings from the Blue Mountains Eye Study. PloS One. 2016;11(1):e0147646. https://doi.org/10.1371/journal.pone.0147646ArticlePubMedPMC
- 9. Wallhagen MI, Strawbridge WJ, Shema SJ, Kurata J, Kaplan GA. Comparative impact of hearing and vision impairment on subsequent functioning. Journal of the American Geriatrics Society. 2001;49(8):1086–1092. https://doi.org/10.1046/j.1532-5415.2001.49213.xArticlePubMed
- 10. Gauthier S, Reisberg B, Zaudig M, Petersen RC, Ritchie K, Broich K, et al. Mild cognitive impairment. The Lancet. 2006;367(9518):1262–1270. https://doi.org/10.1016/S0140-6736(06)68542-5Article
- 11. Harrabi H, Kergoat MJ, Rousseau J, Boisjoly H, Schmaltz H, Moghadaszadeh S, et al. Age-related eye disease and cognitive function. Investigative Ophthalmology & Visual Science. 2015;56(2):1217–1221. https://doi.org/10.1167/iovs.14-15370Article
- 12. Teipel S, Fritze T, Ovari A, Buhr A, Kilimann I, Witt G, et al. Regional pattern of dementia and prevalence of hearing impairment in Germany. Journal of the American Geriatrics Society. 2015;63(8):1527–1533. https://doi.org/10.1111/jgs.13561ArticlePubMed
- 13. Wood J, Chaparro A, Anstey K, Lacherez P, Chidgey A, Eisemann J, et al. Simulated visual impairment leads to cognitive slowing in older adults. Optometry and Vision Science : Official Publication of the American Academy of Optometry. 2010;87(12):1037–1043. https://doi.org/10.1097/opx.0b013e3181fe64d7ArticlePubMed
- 14. Amieva H, Ouvrard C. Does treating hearing loss in older adults improve cognitive outcomes? A review. Journal of Clinical Medicine. 2020;9(3):805. https://doi.org/10.3390/jcm9030805ArticlePubMedPMC
- 15. Horowitz A, Reinhardt JP, Boerner K. The effect of rehabilitation on depression among visually disabled older adults. Aging & Mental Health. 2005;9(6):563–570. https://doi.org/10.1080/13607860500193500Article
- 16. Nkyekyer J, Meyer D, Pipingas A, Reed NS. The cognitive and psychosocial effects of auditory training and hearing aids in adults with hearing loss. Clinical Interventions in Aging. 2019;14:123–135. https://doi.org/10.2147/cia.s183905ArticlePubMedPMC
- 17. Bisgaard N, Ruf S. Findings from EuroTrak surveys from 2009 to 2015: Hearing loss prevalence, hearing aid adoption, and benefits of hearing aid use. American Journal of Audiology. 2017;26(3S):451–461. https://doi.org/10.1044/2017_aja-16-0135ArticlePubMed
- 18. Wilson RH, Noe CM, Cruickshanks KJ, Wiley TL, Nondahl DM. Prevalence and degree of hearing loss among males in the Beaver Dam Cohort: Comparison of veterans and nonveterans. Journal of Rehabilitation Research and Development. 2010;47(6):505–520. https://doi.org/10.1682/jrrd.2009.10.0169ArticlePubMedPMC
- 19. Zazove P, Plegue MA, McKee MM, DeJonckheere M, Kileny PR, Schleicher LS, et al. Effective hearing loss screening in primary care: The early auditory referral-primary care study. Annals of Family Medicine. 2020;18(6):520–527. https://doi.org/10.1370/afm.2590ArticlePubMedPMC
- 20. Jenstad L, Moon J. Systematic review of barriers and facilitators to hearing aid uptake in older adults. Audiology Research. 2011;1(1):e25. https://doi.org/10.4081/audiores.2011.e25ArticlePubMedPMC
- 21. Lee SH, Choo NH, Kim HJ. Although Korea's aging rate is the fastest, the poverty rate for the elderly already ranks the first in the OECD. Korea Economic Research Institute Post. 2021 February [cited 2023 Jan 3] Available from: http://www.keri.org/web/www/news_02?p_p_id=EXT_BBS&p_p_lifecycle=0&p_p_state=normal&p_p_mode=view&_EXT_BBS_struts_action=%2Fext%2Fbbs%2Fview_message&_EXT_BBS_messageId=356132
- 22. Ministry of Health and Welfare. Project to Prevent and Manage Blindness for the Elderly [Internet]. Sejong: Ministry of Health and Welfare. 2017 [cited 2023 Jan 21]. Available from: http://www.mohw.go.kr/react/policy/index.jsp?PAR_MENU_ID=06&MENU_ID=06390103&PAGE=3&topTitle=
- 23. Chae SW. A Study on the application of National Health Insurance Service to the hearing aids in the hearing impaired elderly. Research Report. Wonju: National Health Insurance Service; 2020. Report No.: 2020-2-0005.
- 24. Liu H, Zhang Y, Burgard SA, Needham BL. Marital status and cognitive impairment in the United States: Evidence from the National Health and Aging Trends Study. Annals of Epidemiology. 2019;38:28–34. https://doi.org/10.1016/j.annepidem.2019.08.007ArticlePubMedPMC
- 25. Barnes LL, De Leon CFM, Wilson RS, Bienias JL, Evans DA. Social resources and cognitive decline in a population of older African Americans and whites. Neurology. 2004;63(12):2322–2326. https://doi.org/10.1212/01.wnl.0000147473.04043.b3ArticlePubMed
- 26. Zunzunegui MV, Alvarado BE, Del Ser T, Otero A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. The Journals of Gerontology. Series B: Psychological Sciences and Social Sciences. 2003;58(2):S93–S100. https://doi.org/10.1093/geronb/58.2.s93Article
- 27. Lee WJ, Kim HG, Kim H, Yoo SR, Jang SE, Oh MK. Tangible social support and cognitive decline in the elderly: The Korean longitudinal study of aging. Korean Journal of Family Practice. 2017;7(3):337–341. https://doi.org/10.21215/kjfp.2017.7.3.337Article
- 28. Verbrugge LM, Jette AM. The disablement process. Social Science & Medicine (1982). 1994;38(1):1–14. https://doi.org/10.1016/0277-9536(94)90294-1Article
- 29. Kang YW, Na DL, Hahn SH. A validity study on the Korean Mini-Mental State Examination(K-MMSE) in dementia patients. Journal of the Korean Neurological Association. 1997;15(2):300–308.
- 30. House JS. Work stress and social support. 1st ed. Boston MA: Addison-Wesley Pub. Co., Reading, Mass; 1981. 156 p.
- 31. Brown SL, Nesse RM, Vinokur AD, Smith DM. Providing social support may be more beneficial than receiving it: Results from a prospective study of mortality. Psychological Science. 2003;14(4):320–327. https://doi.org/10.1111/1467-9280.14461ArticlePubMed
- 32. Väänänen A, Buunk BP, Kivimäki M, Pentti J, Vahtera J. When it is better to give than to receive: Long-term health effects of perceived reciprocity in support exchange. Journal of Personality and Social Psychology. 2005;89(2):176–193. https://doi.org/10.1037/0022-3514.89.2.176ArticlePubMed
- 33. Park JS, Lee YW, Kim HS. Cognitive impairment risk factors in elders. Journal of Korean Gerontological Nursing. 2015;17(3):121–130. http://doi.org/10.17079/jkgn.2015.17.3.121Article
- 34. Senger J, Bruscato NM, Werle B, Moriguchi EH, Pattussi MP. Nutritional status and cognitive impairment among the very old in a community sample from southern Brazil. The Journal of Nutrition, Health & Aging. 2019;23(10):923–929. https://doi.org/10.1007/s12603-019-1230-xArticle
- 35. Chen L, Cao Q. Poverty increases the risk of incident cognitive impairment among older adults: A longitudinal study in China. Aging & Mental Health. 2020;24(11):1822–1827. https://doi.org/10.1080/13607863.2019.1663491Article
- 36. Lee HK, Lee KH. Health-related factors influencing cognitive impairment of the elderly in primary health care posts: With focus on eating habits, activities of daily living, alcohol drinking, and smoking. Journal of the Korean Data Analysis Society. 2016;18(2):965–979.
- 37. Hoang TD, Reis J, Zhu N, Jacobs DR JR, Launer LJ, Whitmer RA, et al. Effect of early adult patterns of physical activity and television viewing on midlife cognitive function. JAMA Psychiatry. 2016;73(1):73–79. https://doi.org/10.1001/jamapsychiatry.2015.2468ArticlePubMedPMC
- 38. Muhammad T, Meher T. Association of late-life depression with cognitive impairment: Evidence from a cross-sectional study among older adults in India. BMC Geriatrics. 2021;21(1):364. https://doi.org/10.1186/s12877-021-02314-7ArticlePubMedPMC
- 39. Muhammad T, Govindu M, Srivastava S. Relationship between chewing tobacco, smoking, consuming alcohol and cognitive impairment among older adults in India: a cross‐sectional study. BMC geriatrics. 2021;21(1):1–14. https://doi.org/10.1186/s12877-021-02027-xArticlePubMedPMCPDF
- 40. Gold DA. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. Journal of Clinical and Experimental Neuropsychology. 2012;34(1):11–34. https://doi.org/10.1080/13803395.2011.614598ArticlePubMed
- 41. Lee JE. The relationship between cognitive function and physical health factors in the elderly. Journal of the Korean Gerontological Society. 2022;42(3):481–497. http://doi.org/10.31888/JKGS.2022.42.3.481Article
- 42. Maharani A, Dawes P, Nazroo J, Tampubolon G, Pendleton N. Associations between self-reported sensory impairment and risk of cognitive decline and impairment in the health and retirement study cohort. The Journals of Gerontology: Series B, Psychological Sciences and Social Sciences. 2020;75(6):1230–1242. https://doi.org/10.1093/geronb/gbz043ArticlePubMed
- 43. Lin MY, Gutierrez PR, Stone KL, Yaffe K, Ensrud KE, Fink HA, et al. Vision impairment and combined vision and hearing impairment predict cognitive and functional decline in older women. Journal of the American Geriatrics Society. 2004;52(12):1996–2002. https://doi.org/10.1111/j.1532-5415.2004.52554.xArticlePubMed
- 44. Naël V, Pérès K, Dartigues JF, Letenneur L, Amieva H, Arleo A, et al. Vision loss and 12-year risk of dementia in older adults: The 3C cohort study. European Journal of Epidemiology. 2019;34(2):141–152. https://doi.org/10.1007/s10654-018-00478-yArticle
- 45. Deal JA, Betz J, Yaffe K, Harris T, Purchase-Helzner E, Satterfield S, et al. Hearing impairment and incident dementia and cognitive decline in older adults: The health ABC study. The Journals of Gerontology. Series A: Biomedical Sciences and Medical Sciences. 2017;72(5):703–709. https://doi.org/10.1093/gerona/glw069Article
- 46. Tomioka K, Okamoto N, Morikawa M, Kurumatani N. Self‐reported hearing loss predicts 5‐year decline in higher‐level functional capacity in high‐functioning elderly adults: The Fujiwara‐Kyo study. Journal of the American Geriatrics Society. 2015;63(11):2260–2268. https://doi.org/10.1111/jgs.13780ArticlePubMed
- 47. Wallhagen MI, Strawbridge WJ, Shema SJ. The relationship between hearing impairment and cognitive function: A5-year longitudinal study. Research in Gerontological Nursing. 2008;1(2):80–86. https://doi.org/10.3928/19404921-20080401-08ArticlePubMed
- 48. Evans IEM, Martyr A, Collins R, Brayne C, Clare L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. Journal of Alzheimer's Disease : JAD. 2019;70(s1):S119–S144. https://doi.org/10.3233/jad-180501Article
- 49. Tseng YC, Gau BS, Liu TC, Hsieh YS, Huang GS, Lou MF. Association between sensory impairments and restricted social participation in older adults: A cross-sectional study. Collegian. 2022;29(6):850–859. https://doi.org/10.1016/j.colegn.2022.06.002Article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite