
Articles
- Page Path
- HOME > J Korean Acad Community Health Nurs > Volume 33(3); 2022 > Article
- Original Article The Effects of Non-pharmacological Interventions on Sleep among Older Adults in Korean Long-term Care Facilities: A Systematic Review and Meta-analysis
- Sun Ok Jung, Hye Young Kim, Eun Ju Choi
-
DOI: https://doi.org/10.12799/jkachn.2022.33.3.340
Published online: September 30, 2022

- 871 Views
- 63 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
This study aimed to examine the effects of non-pharmacological sleep intervention programs in improving sleep quality among older adults in long-term care facilities.
Methods: A literature search and selection was performed on nine different databases using the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Overall, 14 studies met the inclusion criteria and were systematically reviewed. For the metaanalysis, the effect size was estimated using the random-effects model in Review Manager (RevMan) desktop version 5.4 of the Cochrane Library.
Results: The meta-analysis of overall non-pharmacological interventions obtained a total effect size of 1.0 (standardized mean difference [SMD]=1.0, 95% confidence interval [CI]: 0.64~1.35), which was statistically significant (Z=5.55, p<.001). The most frequently studied non-pharmacological intervention was aroma therapy, with an effect size of 0.61 (SMD=0.61, 95% CI: 0.14~1.08), which was statistically significant (Z=2.55, p=.010). In the subgroup analysis, group-based interventions, interventions for >4 weeks, and untreated control studies were more effective.
Conclusion: This study confirms that non-pharmacological interventions are effective in improving sleep quality among older adults in long-term care facilities. However, the sample size was small and the risk of bias in assessing the interventions of individual studies was unclear or high, thereby limiting the generalizability of the results. Further reviews that evaluate randomized control trials, evidence-based interventions that consider older adult participants' physical activity levels, different intervention methods and durations, and different control group intervention types are needed to obtain more conclusive evidence.
| J Korean Acad Community Health Nurs. 2022 Sep;33(3):340-355. English. Published online Sep 30, 2022. https://doi.org/10.12799/jkachn.2022.33.3.340 | |
| © 2022 Korean Academy of Community Health Nursing | |
Sun Ok Jung ,
Hyeyoung Kim
and Eunju Choi ,
Hyeyoung Kim
and Eunju Choi
| |
| Graduate Student, College of Nursing, Ewha University, Seoul, Korea. | |
Corresponding author: Choi, Eunju. College of Nursing, Ewha University, 52 Ewhayeodae-gil, Seodaemun-gu, Seoul 03760, Korea. Tel: +82-63-261-4528, Fax: +82-2-3277-2876, | |
| Received April 28, 2022; Revised August 27, 2022; Accepted September 01, 2022. | |
|
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
Purpose
This study aimed to examine the effects of non-pharmacological sleep intervention programs in improving sleep quality among older adults in long-term care facilities.
Methods
A literature search and selection was performed on nine different databases using the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Overall, 14 studies met the inclusion criteria and were systematically reviewed. For the meta-analysis, the effect size was estimated using the random-effects model in Review Manager (RevMan) desktop version 5.4 of the Cochrane Library.
Results
The meta-analysis of overall non-pharmacological interventions obtained a total effect size of 1.0 (standardized mean difference [SMD]=1.0, 95% confidence interval [CI]: 0.64~1.35), which was statistically significant (Z=5.55, p<.001). The most frequently studied non-pharmacological intervention was aroma therapy, with an effect size of 0.61 (SMD=0.61, 95% CI: 0.14~1.08), which was statistically significant (Z=2.55, p=.010). In the subgroup analysis, group-based interventions, interventions for >4 weeks, and untreated control studies were more effective.
Conclusion
This study confirms that non-pharmacological interventions are effective in improving sleep quality among older adults in long-term care facilities. However, the sample size was small and the risk of bias in assessing the interventions of individual studies was unclear or high, thereby limiting the generalizability of the results. Further reviews that evaluate randomized control trials, evidence-based interventions that consider older adult participants' physical activity levels, different intervention methods and durations, and different control group intervention types are needed to obtain more conclusive evidence. |
|
Keywords:
Review; Sleep; Sleep quality; Aged; Long-term care
|
|
|
INTRODUCTION
|
Sleep disturbance, among older adults, often co-exists with other symptoms and can exacerbate their condition. Several factors, including residents' physical and emotional symptoms, and environmental characteristics of the long-term care facilities (LTCFs), can contribute to sleep disturbance [1]. Physical factors include physical disability, cognitive impairment, chronic disease [1, 2] and decreased activities of daily living (ADL)[3], pain and fatigue, physical activity, and poor self-management [3, 4]. Psychological factors include depression, anxiety, loneliness, worry, and other emotional disturbances [5]. Environmental factors, such as a decrease in physical activity, restriction of social interaction, reduced exposure to sunlight, poor sleep hygiene [2], noise at night, and night lighting, can also interfere with sleep onset and maintenance [3, 6]. Thus, older adults at LTCFs are physically, mentally, and environmentally vulnerable groups owing to their high dependence on ADLs, complex diseases, multi-drug administration, and restrictions on social participation [7, 8]. Therefore, they have more sleep disturbances than community-dwelling older adults owing to the combination of said factors [9]. Studies report that more than one-third of older residents in LTCFs have a sleep disorder [10], and approximately 72% of them have poor sleep quality [11]. The risk of sleep disorders among older residents in LTCFs is higher than that among community-dwelling older adults because of the poor environment and physical factors that affect sleep hygiene.
Multiple studies have reported the negative effects of poor sleep on residents in LTCFs. For instance, sleep disturbances such as breathing difficulties, nightmares, poor sleep quality, and difficulty concentrating during sleep can cause depression in LTCF residents [12, 13]. Furthermore, persistent sleep deprivation can lead to cognitive impairment [14, 15], which is a major factor in re-admission to LTCFs [16]. Changes in sleep patterns can adversely affect neurological health by increasing the risk of dementia [17], leading to decreased functional recovery, social separation, increased risk of falls, and even death [18]. Thus, sleep disorders can have varied effects on the older adults' lives, which highlights the importance of investigating sleep management interventions for residents in LTCFs [19].
Previous evidence suggests that non-pharmacological approaches should be prioritized over drug use for the treatment of sleep disorders in older adults, and drug access is recommended only when non-pharmacological approaches have proved ineffective [20, 21]. However, drugs used for sleep disorders can lead to difficulties with tolerance and dependence [21], and long-term use increases the risk of dementia in older adults [22] and significantly increases the risk of falls [23]. Thus, non-pharmacological interventions including acupressure, auricular acupuncture, behavioral therapy, massage, hand massage, mindfulness meditation, tart cherry juice, sleep education, relaxation, and attention control, should be preferred. These interventions are crucial for improving older adults' sleep quality [24, 25], and it is necessary to establish evidence for their effectiveness in older adults.
Moreover, although systematic reviews of non-pharmacological interventions for older adults in LTCF settings have been conducted in other studies, and results regarding sleep improvement have been identified and evaluated, no meta-analyses have been performed [25, 26]. This could be because meta-analysis is not feasible due to considerable heterogeneity when including various countries and intervention methods. With more than a decade since the introduction of long-term care insurance in 2008, many non-pharmacological interventions for improving sleep have been employed in Korean LTCFs. In Korea, most studies have reported the impact of non-pharmacological interventions in patients with sleep disorders; however, not specifically in older adults [27]. Other studies that performed meta-analyses on the quality of sleep in older adults in the community were limited to physical activity programs [28]. For non-pharmacological interventions, most existing reviews analyzed participants with a specific type of dementia or those in a community setting. To bridge this gap in the existing literature, it is necessary to investigate all types of non-pharmacological interventions for older adults living in LTCFs. Therefore, the aim of this study was to provide a systematic review of the best available evidence for interventions suitable for older adults in Korean LTCFs, by integrating non-pharmacological sleep intervention studies and analyzing their effects.
1. Research Purpose
This study aimed to identify and evaluate the literature related to non-pharmacological sleep interventions for older adults in Korean LTCFs, and to estimate the effect size of different types and methods of intervention programs.
|
METHODS
|
1. Research Design
This study employs a systematic review and meta-analysis to analyze the non-pharmacological sleep interventions' effect among older adults in Korean LTCFs.
2. Study Selection Process
1) Search strategy
This research was exempted from review as a secondary study by the Institutional Review Board. To examine the latest trends in non-pharmacological sleep interventions, we searched for literature published in the last 10 years, after the introduction of long-term care insurance, from January 2011 to April 2021 (last search date was April 13, 2021). We selected the database according to the Core, Standard, and Ideal (COSI) model developed by the National Library of Medicine. We searched five English databases [EMBASE, Cochrane, CINAHL, PubMed, and PsycINFO] extensively for English-language publications, and five Korean databases [Research Information Sharing Service (RISS), Korean Studies Information Service System (KISS), National Digital Science Library (NDSL), Korean Medical Database (KMBASE), and the DataBase Periodical Information Academy (DBPia)]. Furthermore, as per the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) protocol, additional records were identified through other sources, which included article reference lists identified during the primary research stage.
In the primary research stage of this study, if research was identified to be conducted on older adult participants, it was included in the analysis, regardless of any specific age criteria. The search keywords were extensively selected in accordance with PICO questions and literature [29]; participants (P) were older adults living in long-term care facilities, intervention (I) was non-pharmacological interventions, and the outcome variable (O) was sleep quality. Participant (P) keywords were "aged", "older", "elderly", "senior*", "geriatric*", "residential facilities", "long term", "institutional", and "nursing home". Intervention (I) keywords were "cognitive behavioral therapy", "cognitive behavior", "sleep hygiene", "sleep education", "sleep health", "sleep restriction", "stimulus control", "relaxation training", "relaxation", "muscle relaxation", "exercise", "walking", "Tai Chi", "acupuncture", "electroacupuncture", and "auricular acupuncture" as non-pharmacological interventions, and the outcome variable (O) keywords were "sleep", "sleep disorder", "insomnia", "wakeful", and "dyssomnia"(Supplementary Material 1). The same Korean keywords as the English keywords were searched for the Korean literature search.
In this study, the literature selection process was described according to the PRISMA guidelines (Figure 1). A total of 4496 papers were identified through database and article references, and 173 papers were selected after excluding duplicate literature (N=458) and non-Korean facilities (N=3,865). After screening titles and abstracts, we reviewed the full text of 26 articles and selected 14 articles that met the inclusion and exclusion criteria (Appendix 1). Among these, only 11 studies were meta-analyzed. The study selection process conducted in this study was independently performed by three researchers, and in cases of disagreement, decision was achieved through consensus after sufficient discussion.
|

2) Eligibility criteria
Material selection was also performed according to the PRISMA guidelines. The inclusion criteria were (1) articles targeting older adults residing in LTCFs in Korea, (2) non-pharmacological intervention studies on sleep, (3) subjective and objective measurements of sleep quality, (4) randomized controlled trials (RCTs), non-randomized controlled trials (NRCTs), single-group pre-post study, and (5) only academic articles. Exclusion criteria were (1) articles for which the full-text, such as abstracts, posters, and conference materials, could not be verified; (2) articles for which the mean and standard deviation were not presented before and after intervention, (3) pharmacological intervention studies, (4) systematic reviews and meta-analyses, and (5) studies in which the research design did not meet the criteria such as pilot studies, reviews, case studies, and correlation studies.
3) Data extraction
We independently extracted data according to the data extraction list prepared to extract the data accurately. Thus, the study's general characteristics, authors, publication year, study type, and study participant characteristics (average age and number of samples) were extracted. Further, we extracted intervention characteristics, such as non-pharmacological intervention type, length of session, frequency, duration, control group intervention, and intervention provider. For the outcome measure, data from the sleep quality measurement scales and the direction of the outcome were extracted. No items were omitted from any study.
3. Risk of Bias Assessment
We conducted a risk of bias assessment of the selected literature to increase the findings' validity. Randomized controlled experimental studies were critically reviewed in seven categories using the Cochrane's Risk of Bias (RoB) tool [30], whereas other quasi-experimental studies were assessed using the Risk of Bias Tool for Non-Randomized Studies version 2.0 (RoBANS) [30]. The risk of bias assessment of the literature was conducted independently by three researchers, and during disagreements a consensus was reached through sufficient discussion. The risk of bias assessment results were entered into Review Manager (RevMan) to present the overall assessment results for that specific risk.
4. Statistical Analyses
1) Characteristics of selected literatures
General characteristics of the selected literatures and characteristics of the non-pharmacological interventions were analyzed using descriptive statistics (frequency, percentage, and mean). The direction of the study results was analyzed as "positive" if the intervention had a statistically significant effect on sleep quality in an individual study, and "negative" if there was no statistically significant effect.
2) Effect size of selected literatures
We used RevMan version 5.4 to analyze the effect size; subgroup analysis was performed when three or more studies were conducted in the same subgroup. The individual studies' homogeneity was confirmed using the Higgins' I2 test and Cochran's χ2 test. The I2 value was evaluated as "low heterogeneity at 25%", "medium heterogeneity at 50%", and "high heterogeneity at 75% or higher" [31]. Considering the great diversity of non-pharmacological interventions for the older adults residing in LTCFs and the high clinical and research methodological diversity of the intervention application environment, the effect size was analyzed using a random effect model.
The effect size was calculated using the mean, standard deviation, and number of samples. The standardized mean difference was calculated considering the diversity of tools used in individual studies. The effect size was evaluated at 95% confidence interval and 5% significance level. The criteria for effect size interpretation were 0.2~0.5 as small effect, 0.5~0.8 as medium effect, and 0.8 or more as large effect [32].
3) Publication bias
To verify publication bias, visual analysis was performed through a funnel plot, and trim-and-fill analyses were conducted using Comprehensive Meta-Analysis (CMA) 3.0 (Biostat, Englewood, NJ, USA). An evenly distributed scatter plot suggested no publication bias. Egger's linear regression test was used to determine whether the funnel plot was symmetrical by setting the significance level to .05 [33].
|
RESULTS
|
1. Characteristics of Selected Literature
Table 1 shows the characteristics of the 14 selected studies. Among them, one was an RCT, 11 were NRCTs, and two were single-group pre-post studies. Among the non-pharmacological intervention programs, aroma therapy was the most commonly used (n=5; RCT=1, NRCT=4). Although various interventions such as cognitive behavioral intervention and phototherapy are being tested abroad [34], most of the intervention studies conducted in Korea, have mainly focused on complementary and alternative therapies such as massage, aromatherapy, laughter therapy, and auricular acupressure therapy. Recently, attempts have been made to measure sleep quality through objective as well as subjective measurements, as a result of these interventions. Session length varied from 10 min to 90 min; most interventions were within 30 min (50%). The intervention duration ranged from 3~74 days, a majority of the studies had an intervention with a duration of 4 weeks or less (n=9, 64.3%). Intervention providers were mostly researchers or research assistants, but in one study [35], the participants themselves conducted the aroma inhalation intervention, and the nurse in the LTCF ensured it. Regarding control groups, nine studies (64.3%) did not implement any intervention. Moreover, one of RCT and eight of NRCTs (64.3%) measured sleep quality using the self-reported Korean Sleep Scale (KSS) developed by Oh et al. [36]. The publication years were distributed from 2011 to 2020, and all studies were original articles. Interventions were conducted in LTCFs (n=10), geriatric hospitals (n=3), and welfare facilities (n=1). The number of participants in experimental and control groups in the individual studies ranged from 3~30; the total number of participants from all 14 studies was 563, with 251 in the experimental group and 264 in the control group; the sample size in the two single-group pre-post study was 48.
|

The two single-group pre-post studies utilized biomarkers to confirm sleep quality. For the occupation-based sleep intervention program, the effectiveness of sleep quality was showed by measuring sleep efficiency using a smartwatch. Aroma head and neck massage used physiological indicators such as serotonin, cortisol, blood pressure, and pulse, to confirm the increase in serotonin, decrease in cortisol, and decrease in systolic and diastolic blood pressure, which are objective indicators of improved sleep quality. In comparison to assessing sleep quality using a subjective measurement tool, an objective measurement tool provides a more accurate measure of sleep quality. Based on the single-group pre-post study, NRCT and RCT studies including biomarker measurements and control groups are needed in the future.
2. Risk of Bias Assessment
The risk of bias assessment results are as follows (Figure 2A, 2B). For the one RCT study in our sample, blinding for allocation concealment and outcome assessment was not mentioned, and thus, it was evaluated as an uncertain or unclear risk. As blinding of participants' and personnel information was not performed, the risk of bias was evaluated to be high. An analysis of bias risk in the 11 NRCT studies and two single-group pre-post studies revealed that the possibility of target group comparison bias was low in all 12 studies; one study [37] did not mention these details, and thus, it was evaluated as being subject to unclear risk. In two articles [37, 38] with an intervention period of two months or longer, the risk of confounding bias was evaluated as high because it was judged that the bias would occur due to natural processes and learning effects. Regarding blinding of assessor bias, six studies that were not blinded were evaluated as high-risk, and seven studies without the mention of blinding were evaluated as having unclear risk. As for incomplete outcome data bias, one study [39], which did not provide the correct number of samples in the outcome table, was evaluated as having unclear risk. Selective outcome reporting bias risk was evaluated as low in all studies except for one [38], which did not report the results corresponding to the study's purpose.
|

3. Effect of Non-pharmacological Interventions on Sleep Quality
1) Effect size of non-pharmacological interventions on sleep quality
Of the 14 studies, 11 studies measuring sleep quality using self-reported subjective scales were analyzed, excluding the two single-group studies with different study designs, and one study in which outcome variables were measured using an objective scale. Non-pharmacological interventions increased sleep quality in the experimental group by 1.0 (SMD=1.0, 95% CI: 0.64~1.35) compared to the control group, and the effect was statistically significant (Z=5.55, p<.001) (Figure 3).
|

2) Effect size of aromatherapy on sleep quality
Four studies (A1, A2, A3, and A4) used aromatherapy as the non-pharmacological intervention (I2=56%, χ2=6.81, df=3, p=.08). The aromatherapy's effective size was increased by 0.61 (SMD=0.61, 95% CI: 0.14~1.08) in the experimental group compared to the control group, and the effect was statistically significant (Z=2.55, p=.01).
3) Sleep quality effect size according to individual vs. group interventions
Subgroup analysis was performed using individual vs. group interventions (Table 2, Appendix 2). Seven studies conducted individual interventions (I2=65%, χ2=17.15, df=6, p=.009), and four studies conducted group interventions (I2=73%, χ2=11.13, df=3, p=.01). In individual interventions, sleep quality increased by 0.82 (SMD=0.82, 95% CI: 0.42~1.21) in the experimental group compared to the control group, and the effect was statistically significant (Z=4.07, p<.001). For group interventions, sleep quality increased by 1.37 [SMD=1.37, 95% CI: 0.66~2.08) in the experimental group compared to the control group, and the effect was statistically significant (Z=3.80, p<.001).
|

4) Sleep quality effect size according to intervention duration
To compare the effect size according to the intervention duration, a subgroup analysis was performed using a random effects model (Table 2, Appendix 2). Studies with interventions duration of 4 weeks or less showed low heterogeneity (within 4 weeks: I2=29%, χ2=8.45, df=6, p=.21), whereas the studies with interventions more than 4 weeks showed homogeneity (over 4 weeks: I2=0%, χ2=1.01, df=3, p=.80). When the intervention duration was less than 4 weeks, it increased sleep quality by 0.64 (SMD=0.64, 95% CI: 0.37~0.91), with the effect being statistically significant (Z=4.71, p<.001). Meanwhile, when the intervention's duration was more than 4 weeks, it increased sleep quality by 1.69 (SMD=1.69, 95% CI: 1.32~2.06), with the effect being statistically significant (Z=8.86, p<.001).
5) Sleep quality effect size according to control intervention
A subgroup analysis was performed to compare the magnitude of the effect on sleep quality between the sham intervention studies and the untreated control studies (Table 2, Appendix 2). The three sham intervention studies showed low heterogeneity (I2=22%, χ2=2.56, df=2, p=.28), whereas the eight untreated control studies showed moderate heterogeneity (I2=55%, χ2=15.67, df=7, p=.03). In the sham intervention studies, the experimental group's effect size was 0.39 (SMD=0.39, 95% CI: 0.01~0.77), with the effect being statistically significant (Z=1.99, p=.05). Meanwhile, in the untreated control studies, the effect size was 1.23,(SMD=1.23, 95% CI: 0.87~1.58), which was statistically significant (Z=6.71, p<.001).
4. Publication Bias
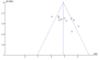
Analysis of publication bias using a funnel plot confirmed that the results were not symmetric (Figure 4). Egger's linear regression test, which objectively verifies publication bias through statistical significance, revealed a bias coefficient of 2.42 (t=0.74, df=8, p=.23), confirming the absence of publication bias. Publication bias was corrected by inserting one study estimated by the Trim and Fill method, an exploratory sensitivity analysis method. The bias-corrected average effect size was calculated at 0.95, which was reduced from the pre-calibration average effect size of 1.04; however, it can be interpreted that the 95% CI of the bias-corrected effect size is not a statistically significant error to 0.52~1.36.
|
|
DISCUSSION
|
This study investigated the effects of non-pharmacological sleep interventions among older adults in Korean LTCFs. In this review, we included one RCT, 11 NRCTs (78.6%), and 2 single-group pre-post studies. The results indicated that the RCT research was limited, possibly because it was difficult to create a controlled environment as required for randomized experimental studies in Korean LTCFs [40].
Among the types of non-pharmacological interventions, the most common interventions are those with aromatherapy with five studies (28.6%), possibly because aromatherapy can be used in multiple ways, such as skin application, inhalation, and massage [41], and can be safely applied to older adults without serious complications [42]. Meanwhile, in other countries, physical activity interventions, such as high-intensity physical strength training, walking, and elastic band exercises, have been implemented to improve sleep quality [43]. In Korea, there have been few physical activity interventions owing to the limited environment for patient safety management.
The most common intervention characteristics were intervention time of 30~60 minutes (six articles, 42.8%), intervention frequency of once a week (three articles, 21.4%), and a total intervention period of 4~8 weeks (six articles, 42.8%). These findings are consistent with previous studies where interventions were performed typically for 30~60 minutes per session, once a week, for a total of 4~8 sessions [44]. Furthermore, the improvement of sleep quality was confirmed in 12 articles (85.7%). Therefore, it can be inferred that non-pharmacological interventions are effective in improving sleep quality.
According to the meta-analysis results of 11 articles, an effect size of 1.0 was obtained, which indicates a very large intervention effect. Direct comparison was not possible, as no other study has analyzed the effect of non-pharmacological sleep interventions on older adults in Korean LTCFs. Chae et al. [45] reviewed studies investigating sleep disturbance intervention in cancer patients; Hedges' g was.78, with a medium effect size. Regarding the intervention type, music intervention showed the largest effect size, followed by massage, exercise (walking), and aroma therapy. Meanwhile, Chung and Park [46] meta-analyzed the effects of non-pharmacological interventions on adults with sleep disorders in Korea; Hedges' g was 2.36, indicating a large effect size. Among intervention types, auricular acupuncture therapy showed the largest effect size, followed by foot reflexology massage, aromatherapy, and laughter therapy. Previous studies have indicated that non-pharmacological interventions to improve sleep quality are effective; however, the most effective intervention type differs for each participant [47].
In this study, the aromatherapy's effect on sleep quality showed a medium effect size, whereas Lin et al. [48]'s study with adults over 20 years of age showed a large effect size. Therefore, aromatherapy can be regarded as effective in improving sleep quality. However, aroma therapy tends to show different effects depending on the intervention method; for instance, it has been reported that aroma inhalation therapy has a larger effect size than other application methods, such as massage or intake [41]. Herein, the one study on aroma inhalation could not be confirmed through subgroup analysis. Therefore, it is necessary to compare the effects of inhalation, non-inhalation, and mixing methods in future intervention studies [42].
As in the study of Kim and Oh [34], the effect size by group vs. individual interventions confirmed that group-based interventions had a larger effect size than individual interventions. While individual interventions were centered on physical approaches, in group interventions, interactions with other participants were made, and therefore, psychosocial effects are thought to be involved. This is similar to previous studies where a psychosocial approach was found to be effective for sleep intervention for older adults in a facility [49]. Furthermore, psychological approaches can induce physical relaxation that effectively alleviates physical symptoms [50].
A subgroup analysis was performed for the intervention period (within 4 weeks vs. more than 4 weeks); interventions within 4 weeks showed a medium effect size, whereas interventions longer than 4 weeks showed a very large effect size. Previous studies have reported similar findings with continuous interventions for 4 to 8 weeks after the start of intervention [51, 52]. Additionally, in 10 of 11 articles included in the meta-analysis, sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI) and KSS. The PSQI and KSS assess sleep disorders based on the "last one month;" thus, they are inappropriate for testing the effectiveness of interventions of less than four weeks [51], and it is thought that these results have been reflected. Therefore, for future intervention studies, it is necessary to plan an intervention period that can sufficiently secure the outcome measurement tool's validity or to select a measurement tool suitable for interventions of less than four weeks. Furthermore, most non-pharmacological interventions with an intervention period of more than 4 weeks were group interventions, such as Korean dance, mindfulness meditation, and therapeutic recreation. Therefore, it can be inferred that group intervention and intervention period exceeding 4 weeks had a mutual effect, and thus, the effect size should be interpreted accordingly. Additionally, this study analyzed only the intervention period because of the high heterogeneity in intervention time, frequency, and total sessions among the intervention methods. Thus, it is necessary to analyze the various aspects of intervention methods in the future.
As for improvement in sleep quality by control intervention type (sham intervention group vs. no treatment group), the experimental and sham intervention group showed a small effect size, whereas the experimental and no treatment group showed a very large effect size. As there are limited studies analyzing the effect size according to control intervention type, it is necessary to establish a clear rationale by repeatedly confirming the effect size for the control group intervention types in the future.
Certain limitations of this review would encourage further research. First, the effect size may be overestimated, as 10 of the 11 meta-analyzed articles employed NRCT interventions. Second, generalization is limited, as certain studies had an unclear or high risk of bias, for instance, non-blinding of assessors. Therefore, we suggest further randomized control studies targeting older adults in LTCFs, and a more objective and clear effect size should be established based on future RCT studies. Third, although there were various types of non-pharmacological interventions in the selected literature, there was a limit to analyzing the effect size for each intervention type, because the number of studies for each intervention type was insufficient for a subgroup analysis, except for aroma therapy. Moreover, the number of studies that measured objective sleep quality among the selected studies was insufficient; thus, the size of intervention effect on objective outcomes such as sleep time, sleep efficiency, and sleep-onset delay could not be estimated. Therefore, in future studies, it is recommended to objectively analyze sleep quality using objective measurement tools, such as actigraphy. Fourth, in the case of subgroup analysis according to the study design in other intervention types, there is a limitation in generalization because heterogeneity is rather high. Finally, a mixed analysis of NRCT and RCT showed a positive effect; however, the results of one RCT in our review did not report a statistically significant difference. Consequently, it limited the possibility to draw a clear conclusion about the intervention effect. Therefore, it is recommended that more RCTs be included in future studies.
|
CONCLUSION
|
The results of this systematic review and meta-analysis confirmed the possibility of non-pharmacological interventions affecting the improvement of sleep quality in the older adults in Korea LTCFs. The most frequently used non-pharmacological intervention was aromatherapy, used in five studies. The subgroup analysis revealed that group-based interventions and interventions ≥4 weeks were more positively associated with sleep quality. Therefore, further research investigating the different intervention types, durations, and control groups is needed to improve our understanding of sleep intervention for older adults in LTCF settings. Moreover, further studies are required to provide the best evidence for the standardization and effectiveness of specific interventions, along with detailed analyses of their feasibility in LTCFs in Korea.
|
Appendix 1
|
Analyzed Studies
A1. Park MJ, Park H. Is Hand Massage with the Preferred Aroma Oil better than Lavender on Stress and Sleep for Long-term Care Facility Residents? Korean Journal of Adult Nursing. 2019;31(2):156-164. https://doi.org/10.7475/kjan.2019.31.2.156
A2. Roe SY, Kim KH. Effects of Aroma Massage on Pruritus, Skin pH, Skin Hydration, and Sleep in Elders in Long-term Care Hospitals. Journal of Korean Academy of Nursing. 2013;43(6):726-735. https://doi.org/10.4040/jkan.2013.43.6.726
A3. Ko YJ. Effects of lavender fragrance inhalation method on sleep, depression, and stress of institutionalized elderly. Journal of East-West Nursing Research. 2012;18(2):74-80. https://doi.org/10.14370/jewnr.2012.18.2.074
A4. Lee SY. Effects of aromatherapy hand massage on anxiety, depression, sleep disturbance, and fatigue of the institutionalized elderly. Journal of Korean Biological Nursing Science. 2011;13(1):29-36.
A5. Hong SJ, Kim EH. Effects of aroma head and neck massage on sleep disturbance and problematic behaviors, depression, blood serotonin, blood cortisol, and the vital signs on elders with dementia. Crisisonomy. 2014;10(9):75-92.
A6. Kim HJ, Lee Y, Sohng KY. The effects of footbath on sleep among the older adults in nursing home: a quasi-experimental study. Complementary Therapies in Medicine. 2016;26:40-46. https://doi.org/10.1016/j.ctim.2016.02.005
A7. Seo HS, Sohng KY. The effect of footbaths on sleep and fatigue in older Korean adults. Journal of Korean Academy Fundamentals of Nursing. 2011;18(4):488-496.
A8. Chang E, Park H. Effects of auricular acupressure therapy on musculoskeletal pain, depression and sleep of the elderly in long-term care facilities. Journal of Korean Academy of Community Health Nursing. 2018;29(2):133-142. https://doi.org/10.12799/jkachn.2018.29.2.133
A9. Uhm DC, Nam MJ. Effects of upper meridian massage on cerebral blood flow, emotions, and sleep of the institutionalized elderly. Journal of Korean Academy of Nursing. 2014;6(2):171-180. https://doi.org/10.7475/kjan.2014.26.2.171
A10. Jeon HJ. Effects of Korean dance therapy program on the life stress and sleep quality of elderly dementia patients. The Korean Journal of Physical Education. 2017;56(6):447-457. https://doi.org/10.23949/kjpe.2017.11.56.6.31
A11. Lee MS, Cho BJ. Effects of the brain waves according to participation in therapeutic recreation programs on the depression, sleep disturbance and quality of life in the elderly with dementia. Journal of the Korea Academia-Industrial cooperation Society. 2015;16(8):5096-5110. https://doi.org/10.5762/KAIS.2015.16.8.5096
A12. Kim KN, Son HG, Park HJ. Effects of mindfulness meditation program on sleep, depression, and quality of life in the institutionalized elderly women. The Korean Journal of Health Service Management. 2014;8(3):157-168. https://doi.org/10.12811/kshsm.2014.8.3.157
A13. Seo S, Chang S. Effect of laughing therapy on sleep, depression and self-esteem of elderly women in senior home. Journal of Regional Studies. 2011;19(4):211-225.
A14. Lee HJ, Cha SM. The effects of occupation-based sleep intervention program (OBSP) for inpatients in elderly: a single case study. Korean Aging Friendly Industry Association. 2020; 12 (2):177-187. https://doi.org/10.34264/jkafa.2020.12.2.177

|
References
|
 Cite
Cite
