
Articles
- Page Path
- HOME > J Korean Acad Community Health Nurs > Volume 33(2); 2022 > Article
- Original Article Influencing Factors on Health-related Quality of Life among Japanese Middle-aged Marriage-based Immigrant Women in South Korea: A Cross-Sectional Study
- Keiko Asami, Duck Hee Chae
-
DOI: https://doi.org/10.12799/jkachn.2022.33.2.188
Published online: June 30, 2022

2Associate Professor, College of Nursing, Chonnam National University, Gwangju, Korea
- 614 Views
- 23 Download
- 1 Crossref
- 0 Scopus
Abstract
Purpose
With the first generation of marriage-based immigrant women in East Asia now reaching their middle or old age, the need to focus investigations on their health-related quality of life has arisen. This study aimed to examine the extent to which physical and mental health, and psychosocial variables can predict health-related quality of life among Japanese middle-aged immigrant women.
Methods This study has a descriptive cross-sectional design. A convenience sample of 197 Japanese middle-aged marriage-based immigrant women from two regions of South Korea were recruited between December 2017 and March 2018. Participants completed self-administered questionnaires on health-related quality of life, menopausal symptoms, depression, perceived health status, disease morbidity, social support, and acculturation. The data were analyzed using hierarchical multiple regression.
Results Depression was the strongest predictor of health-related quality of life, followed by perceived health status, social support, and household income. Menopausal symptoms, presence of disease, and acculturation appeared to have no additional impact on participant’s health-related quality of life.
Conclusion In times of rapid growth of global migration and the aging of immigrants in new destination countries, nursing interventions and public health policies for aging marriage-based immigrant women should be prioritized to improve their mental health by facilitating social support and disease management. In addition, social and employment policies that can help immigrant women transition to a healthy midlife are needed.
| J Korean Acad Community Health Nurs. 2022 Jun;33(2):188-195. English. Published online Jun 30, 2022. https://doi.org/10.12799/jkachn.2022.33.2.188 | |
| © 2022 Korean Academy of Community Health Nursing | |
Keiko Asami ,1
and Duckhee Chae2 ,1
and Duckhee Chae2
| |
|
1Graduate Student, College of Nursing, Chonnam National University, Gwangju, Korea. | |
|
2Associate Professor, College of Nursing, Chonnam National University, Gwangju, Korea. | |
Corresponding author: Chae, Duckhee. College of Nursing, Chonnam National University, 160 Baekseo-ro, Dong-gu, Gwangju, 61469, Korea. Tel: +82-62-530-4942, Fax: +82-62-530-4544, | |
| Received February 17, 2022; Revised May 19, 2022; Accepted May 19, 2022. | |
|
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
Purpose
With the first generation of marriage-based immigrant women in East Asia now reaching their middle or old age, the need to focus investigations on their health-related quality of life has arisen. This study aimed to examine the extent to which physical and mental health, and psychosocial variables can predict health-related quality of life among Japanese middle-aged immigrant women.
Methods
This study has a descriptive cross-sectional design. A convenience sample of 197 Japanese middle-aged marriage-based immigrant women from two regions of South Korea were recruited between December 2017 and March 2018. Participants completed self-administered questionnaires on health-related quality of life, menopausal symptoms, depression, perceived health status, disease morbidity, social support, and acculturation. The data were analyzed using hierarchical multiple regression.
Results
Depression was the strongest predictor of health-related quality of life, followed by perceived health status, social support, and household income. Menopausal symptoms, presence of disease, and acculturation appeared to have no additional impact on participant’s health-related quality of life.
Conclusion
In times of rapid growth of global migration and the aging of immigrants in new destination countries, nursing interventions and public health policies for aging marriage-based immigrant women should be prioritized to improve their mental health by facilitating social support and disease management. In addition, social and employment policies that can help immigrant women transition to a healthy midlife are needed. |
|
Keywords:
Depression; Immigrants; Middle-aged; Social support; Quality of life
|
|
|
INTRODUCTION
|
Marriage-based immigration, predominantly of female immigrants, has been a major driver of intra-Asian migration, especially in Japan, Taiwan and South Korea (hereafter Korea) [1]. In Korea, marriage-based immigration began in the 1980s, majority of which were between Japanese women and Korean men. Subsequently, it expanded to women from China and South-East Asia [2]. Marriage-based immigrant women (MIW) generally face difficulties, such as social prejudice, linguistic and cultural differences, child-rearing, and financial hardships [3]. A systematic review study reported that MIW in Korea showed relatively poor health outcomes [4].
The “healthy immigrant effect” is observed when immigrants tend to be healthier than the majority population in host countries [5]. However, those health benefits are not consistent. As the length of immigrants’ stay increase, their health status becomes similar to that of the natives; further, in old age, they show poorer health status than the locals [5, 6]. Recently, more than 45% of MIW in Korea reached the age of 40 or older [7]. The Korean government has provided targeted policies for MIW to effectively fulfill their expected social reproductive roles [8]. As the aging of MIW becomes visible, more attention is needed not only on their social reproductive but also on a more comprehensive health-related quality of life (HRQOL). HRQOL is a multi-dimensional concept that includes domains related to physical, mental, emotional, and social functioning [9]. Midlife transitions, such as menopause, negatively affect their quality of life [10].
In Korea, there has been a sharp increase over the past decade in research on the health of MIW [4, 11]. A recent meta-analysis showed that various studies attempted to identify the factors affecting the quality of life of MIW [11]; these factors included physical and mental health (depression, perceived health status) and psychosocial variables (social support, acculturation). However, the study subjects of most studies were young MIW in their 20s or 30s. Studies on the health of middle-aged MIW are, thus, scarce.
Japanese MIW occupy a unique position among MIW in Korea. Both counties have a relatively homogeneous race and culture and a socio-cultural background influenced by Confucianism [3]. Additionally, while other MIW came from developing countries for financial reasons, Japan was a developed country, with most Japanese migrating for religion-related reasons [3]. Furthermore, Japanese MIW perceived their quality of life to be lower than other MIW [12]. Indeed, the previous studies [12] reported that Japanese MIW were more vulnerable than others, with a low quality of life. However, sample in the previous studies [12, 13] were numerically small, with younger age groups that did not encompass the adequate scope of middle-aged Japanese MIW. It is important to note that Japanese women are a representative group of early MIW in Korea, with most being over the age of 40. Thus, further studies on middle-aged Japanese MIW can be the references to predict the HRQOL of the younger-generation MIW.
Therefore, the purpose of the present study was to identify the extent to which physical and mental health, as well as psychosocial variables can predict HRQOL among Japanese middle-aged MIW in Korea. The study can provide the evidence necessary for future interventions and policymaking to improve the HRQOL of middle-aged MIW.
|
METHODS
|
1. Study Design and Participants
This study used a descriptive, cross-sectional design. Using convenience and snowball sampling, we recruited Japanese MIW living in Gwangju City and Chonnam Province, Korea. To be eligible, participants had to be 40 to 64 years old and able to complete the self-report questionnaire. According to power analysis calculation [14] using G*Power 3.1.9.2, a sample size of at least 166 would be required to give the study power of .95, p value of .05, medium effect size of .15, and 9 predictors. In this study, a mail survey method was sequentially used after face-to-face survey to recruit MIW living in rural areas. A total of 53 MIW responded to the face-to-face survey. Considering the high non-response and item non-response rate of the mail survey method, a total of 260 questionaries were sent by mail. Of the 230 MIW who responded to the survey, data from 197 were used for the analysis, excluding 33 with insufficient responses.
2. Measures
The questionnaire was provided in Japanese. Permission was obtained from the original developers and the relevant copyrighted organization. Questionnaires on menopausal symptoms, acculturation, and social support used in this study were translated from the Korean to Japanese. One Japanese person with a bachelor’s degree in psychology from Korea, one Japanese language professor, and the principal investigator of this study, three of whom were fluent in Korean and Japanese, independently translated the questionnaires. A bilingual expert, Japanese language professor, compared and reviewed the Korean versions and the translated Japanese versions. A pilot survey targeting 17 Japanese middle-aged MIW was conducted with the final version of questionnaires and confirmed that there was no difficulty in comprehension. The self-report survey consisted of four parts: (1) HRQOL; (2) physical and mental health variables (menopausal symptoms, depression, perceived health status, disease morbidity, and regular exercise. Exercise was measured by a single question about participation in regular exercise.); (3) psychosocial variables (social support and acculturation); and (4) demographics (age, education, duration of stay in Korea, employment status, household monthly income, parity, and marital status) were administered.
HRQOL was measured using the Functional Assessment of Cancer Therapy-General Population (FACT-GP), version 4 [15]. FACT-GP is based on the 27-item Functional Assessment of Cancer Therapy-General (FACT-G) which has good psychometric properties. The FACT-GP consists of 21 items after removal of 6 items irrelevant for general population from the FACT-G [15]. The FACT-GP consists of four subscales on physical (6 items), social/family (5 items), emotional (4 items), and functional (6 items) well-being. Responses were scored on a 5-point (ranging from 0=not at all to 4=very much). The higher score indicating higher HRQOL. Cronbach’s αs were .77~.88 for four subscales in a previous study [16] and .79~.86 in this study.
Menopausal symptoms were measured using the 11-item Menopause Rating Scale (MRS) [17]. The MRS consists of three subscales: psychological (4 items), somatic (4 items), and urogenital (3 items) symptoms. Responses were scored on a 5-point scale (ranging from 0=none to 4=extremely severe). A total score of 5 or above was classified as having menopausal symptoms [10]. Cronbach’s α was average on .83 [18] and .87 in this study.
Depression was measured using the 20-item Japanese version of the Center for Epidemiologic Studies Depression Scale (J-CES-D) [19]. The J-CES-D consists of four subscales: depressed affect (7 items), positive affect (4 items), somatic and retarded activity (7 items), and interpersonal (2 items). Responses were scored on a 4-point scale (ranging from 0=rarely or none of the time [less than 1 day] to 3=most or all of the time [5~7 days]). Higher scores indicated greater levels of depressive mood in the past week. A total score of 15 or less was normal, and a score of 16 or above was classified as depressed [19]. Cronbach’s α was .79~.84 in a previous study [19] and .88 in this study.
Perceived health status was measured by one item, namely, “what do you think of your health in general?”, scored on a 5-point Likert scale (ranging from 1=very bad to 5=very good); the responses were subsequently collapsed into three categories (good, fair, bad).
Social support was measured using the 26-item Social Support Scale [20]. The scale consists of four subscales: emotional (7 items), informational (6 items), material (6 items), evaluative (6 items), and overall (1 item) social support. Responses were scored on a 5-point (ranging from 1=none of time to 5=all of the time), with higher scores indicating greater social support. Cronbach’s α was .94 in a previous study [20] and .98 in this study.
Acculturation was measured using the 12-item Short Acculturation Scale for Koreans (SAS-K) [21]. The SAS-K consists of three subscales: language use (5 items), media preference (3 items), and ethics and social relations (4 items). Responses were scored on a 5-point scale. In this study, “Korean” was changed to “Japanese”. Cronbach’s α was .93 in a previous study [21] and .75 in this study.
3. Data Collection
Participants from churches, multicultural family centers, social welfare institutions, and self-help groups were recruited. Data collection was carried out from December 2017 to March 2018. The purpose of the study was explained to participants, and participants’ cooperation was requested for data collection. In the face-to-face survey, one researcher explained the study to the participants and collected data. Questionnaires were mailed to potential participants living in remote areas, and completed questionnaires were returned to the researchers. The response rate was 100% for face-to-face interviews, and 67.9% for mailed questionnaires.
4. Ethical Considerations
This study was reviewed and approved by the research ethics committee of Chonnam National University (No. 1040198-170727-HR-054-03). Information concerning the purpose of the study, participant anonymity, and voluntary participation was provided to all participants, and written, informed consent was obtained from all participants. All participants received a gift of 3,000 KRW in remuneration after completing the survey.
5. Data Analysis
Data were analyzed using PASW SPSS version 25.0 (IBM Corp, Armonk, NY, USA). The participants’ general characteristics and other study valuables were computed using descriptive statistics. Mean differences in HRQOL regarding study variables were analyzed using the t-test and analysis of variance. Correlations between study variables were analyzed using Pearson’s correlation coefficient. Hierarchical multiple regression was used to test the regression model.
|
RESULTS
|
1. Characteristics of the Participants
The mean age of the participants was 51.15 years (standard deviation [SD] 5.24), and those who were in their 50s comprised the most common age group (60.8%). Those high school graduation or higher education comprised 50.3%. The mean residence period in Korea was 19.61 years (SD 5.16). The majority of the participants (74.0%) were employed. The majority (40.0%) had monthly household income of less than 2,000,000 KRW. Most (93.2%) were married, and 80.4% had more than two childbirths (Table 1).
|

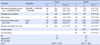
2. Descriptive Statistics of Study Variables
The mean HRQOL score was 57.79 points (SD 11.64). The mean score on the menopausal symptoms scale was 7.23 (SD 7.28); 84.3% had no symptoms. The mean score for depression was 14.11 (SD 7.51); 62.9% were classified as normal, and 37.1% were depressed. The mean score for social support was 82.46 (SD 14.79) and the acculturation score was 37.45 (SD 5.67) (Table 2). Only 11.8% of participants reported that their perceived health status was good, and 26.3% were currently under treatment for certain diseases. Only 15.8% regularly had physical exercise (Table 1).
|
3. HRQOL by Demographics and Study Variables
Women with a monthly household income of less than 2,000,000 KRW had significantly lower HRQOL than those with more than 3,000,000 KRW (F=7.36, p=.001). Poor perceived health status (F=43.18, p<.001), and disease morbidity (t=7.54, p=.007) had significantly lower HRQOL. There was no significant difference in HRQOL in terms of age, duration of stay, educational level, occupation, parity, marital status, and regular exercise (Table 1). There was a positive correlation between HRQOL and social support (r=.64, p<.001) and acculturation (r=.21, p=.003). There was a negative correlation with menopausal symptoms (r=-.39, p<.001) and depression (r=-.75, p<.001) (Table 2).
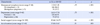
4. Regression Model of HRQOL
As a result of examining the multicollinearity of the independent variables before performing the regression analysis, the tolerance limit ranged from 0.54 to 0.91, and the variance inflation factor was 1.10~1.84. The problem of multicollinearity was not found. The Durbin-Watson was 1.79, confirming the independence of adjacent error terms.
The regression model was tested using hierarchical multiple regression to compare the strength of prediction estimates of the impact of physical and mental health variables (menopausal symptoms, depression, perceived health status, disease morbidity) and psychosocial variables (social support, acculturation) on HRQOL. Household monthly income, physical and mental health variables were entered at Step 1 of the analysis; these accounted for a significant variance in HRQOL, with the explained variance of 70%(F=64.09, p<.001). Depression, perceived health status, and household income were statistically significant. At Step 2, social support and acculturation were introduced into the regression analysis as psychosocial variables, with an additional 5% variance in HRQOL (ΔR2=.05, F=63.18, p<.001). Depression, perceived health status, and household income remained significant, with minor changes in their coefficients. In the final model, which also included psychosocial variables, social support was significantly predictive of HRQOL, with the explained variance of 75% (Table 3).
|
|
DISCUSSION
|
Most countries are increasingly being affected by international migration. Core industrialized countries in East Asia, including Korea, have now emerged as new migration destinations [1]. With the first generation of MIW in East Asia now reaching middle or old age, focused investigations into their HRQOL have become necessary. This study demonstrates that depression is the strongest predictor of HRQOL. Social support, perceived health status, and household income also accounted for significant independent variances in the model. However, menopausal symptoms, disease morbidity, and acculturation did not provide any additional value in predicting HRQOL in Japanese MIW.
Depression is a common mental disorder and a major contributor to the overall global burden of diseases, especially in women [22]. Recent studies have consistently emphasized the importance of mental health interventions in relieving depression, especially for improving HRQOL in older immigrants [22, 23]. In a study of Lee et al. on Korean-Chinese male and female immigrants [24], depression was also the strongest predictor of HRQOL. Among marriage immigrants, 33.4% in their 50s and 42.8% in their 60s reported having experienced depression in the previous year [7]. This is about three to four times higher than that reported by native Koreans in the same age group [25]. This study’s participants were also more depressed than Japanese middle-aged women living in their home countries [26]. In a previous study comparing the prevalence of depression in the first-generation immigrants aged 50 years or older and residents without a history of migration in 11 European countries, the odds ratio for depression in immigrants was 1.42 [22]. Moreover, it should be noted that 37.1% of this group scored 16 or above on the J-CES-D scale, which is indicative of clinically significant depression. This is similar to an earlier study [27], which reported that 30% of elderly Korean immigrants living in the United States had depressive symptoms. While migration may provide opportunities for a better life, the risk of failure, loss, decrease in personal networks, and social values dissimilar to those in the country of origin could negatively affect mental health in immigrants [22]. The process of aging may pose an additional burden for immigrants, which may place them at increased risk for mental health problems.
Our study’s findings indicate that social support is a key protective factor in HRQOL. This is consistent with a systematic review study [4]. In the 2018 Korean National Survey of Multicultural Families [7], 30~40% of the respondents answered that there is no one in Korea to discuss it with or to ask for help, expect for their family members, so there is a high probability that it will be difficult to mobilize appropriate social resources when necessary because social relationships are not developed. One interesting finding is that the social support enjoyed by Japanese MIW was higher than that of middle-aged Korean women [28]. This is contrary to a previous study, which reported that immigrants’ social support is generally weak [27]. It should be noted that most of our study participants were recruited from churches. Agyekum and Newbold reported that the church is important for the quality of life of immigrants, and that religious activities, such as praying, affect the spiritual quality of life [29]. Middle-aged South Asian women who emigrated to Canada reported that attending community support programs facilitated their midlife transition, while limited support from their social circle became a barrier [30]. Therefore, community organizations play a pivotal role in providing strong social solidarity to immigrants for settling and adapting to host countries [29].
Perceived health status was also found to be a significant predictor of HRQOL. This is consistent with a previous study [31]. In a study of HRQOL in Japanese and Australian middle-aged women, physical and mental symptoms were reported to have a negative effect on physical function [31]. While 65.7% of migrant workers who had resided in Korea for more than 10 years perceived their general health as good [6], only 11.8% of this study participants self-reported good health. Among our study’s participants, 65.9% were in their 50s or older, while in Chae et al.’s study, this figure was 43.1%, and 52.7% were male [6]. We assume that majority of this study participants perceived their health to be poor might be related to old age, female gender, and high rates of depressive symptoms.
Household income emerged as a significant predictor of HRQOL. HRQOL of MIW with a monthly household income of less than 2,000,000 KRW was significantly lower than that of MIW with a monthly household income of 3,000,000 KRW or more. Forty percent of the study participants had a monthly household income of less than 2,000,000 KRW-an amount less than half of Korea's average monthly household income [32]. Zou et al. suggest that being employed and possessing adequate life skills can facilitate midlife transition [30]. Although the Korean government has introduced various programs to assist MIW access the labor market, more comprehensive and effective employment and education programs should be prioritized to help MIW integrate into society, as well as to prevent poverty in old age [8, 30].
Although menopausal symptoms and acculturation were not significant in the final regression model, these had a significant relationship with HRQOL in univariate analysis. Acculturation in this study participants was higher than in Korean immigrants living in the United States for 21.7 years [21]. It is known that acculturation starts in early life, and high education level, voluntary migration, and cultural proximity are associated with positive adaptations [33]. In addition, as MIW migrate alone to form families with Koreans, they are fully exposed to the culture of the host country. Similarly, Lee et al. [24] reported that acculturation did not affect the HRQOL of Korean-Chinese immigrants. As acculturation phenomena result from contact between two or more cultures, research on acculturation is complex and must be comparative [33]. Further studies are needed to compare the acculturation of immigrants from diverse ethnic backgrounds and to understand the relationship between acculturation and HRQOL.
Although regular exercise was not a significant predictor of HRQOL, we found a severe lack of exercise among middle-aged MIW. Most of the study participants (84.2%) did not exercise regularly. Anderson and Yoshizawa reported that 36.3% of Japanese middle-aged women did not exercise regularly, and the amount of activity was a significant predictor of HRQOL [31]. Exercise is consistently reported as having an antidepressant effect [34]. It is thus logical that the lack of exercise among our study participants might be associated with a high rate of depressive symptoms.
This study had some limitations. First, only Japanese women living in the two regions were surveyed. Japanese women who voluntarily participated in community activities might have been more active and socially connected. Furthermore, the convenience sample limits the generalizability of our results. Another limitation was that two data collection modes, face-to-face and mail surveys, were used in this study. A preliminary survey was used to confirm that there would be no difficulty in completing the self-administered questionnaire. However, the return rate of the mail survey was only 67.9%, and most data that could not be used in the analysis came from the mail survey due to item non-response. When using mail surveys with immigrants, greater attention should be paid to the questionnaire design stage. In addition, because the cross-sectional nature of the present study, it precludes understanding how the influencing factors of HRQOL among Japanese MIW were changed from immediately after immigrating to Korea to the time of the survey.
Despite these limitations, to the best of our knowledge, this is the first study to examine influencing factors on HRQOL among middle-aged MIW residing in Korea. This study highlights the need for greater attention to the mental health of MIW by nursing researchers, practicing nurses, and policy makers so that timely interventions are implemented and MIW can lead healthy and fulfilling life. Further nursing studies are needed to develop intervention programs for the management of depressive symptoms of immigrant women and evaluate their effectiveness.
|
CONCLUSION
|
Depression is the strongest predictor of HRQOL in Japanese middle-aged MIW. More than a third of MIW had depressive symptoms. Social support, perceived health status, and household income also accounted for significant independent variances in the model. In times of rapid growth in global migration and the aging of immigrants in new migration destination countries, nursing interventions and public health policies for MIW should prioritize improving mental health, building social support, and facilitating disease management. In addition, social and employment policies that can help MIW transition to a healthy midlife are needed.
|
References
|
 Cite
Cite
